Why so many people keep weight loss treatment a secret
06 July, 2026 | Abdul Jabbar - MPharm

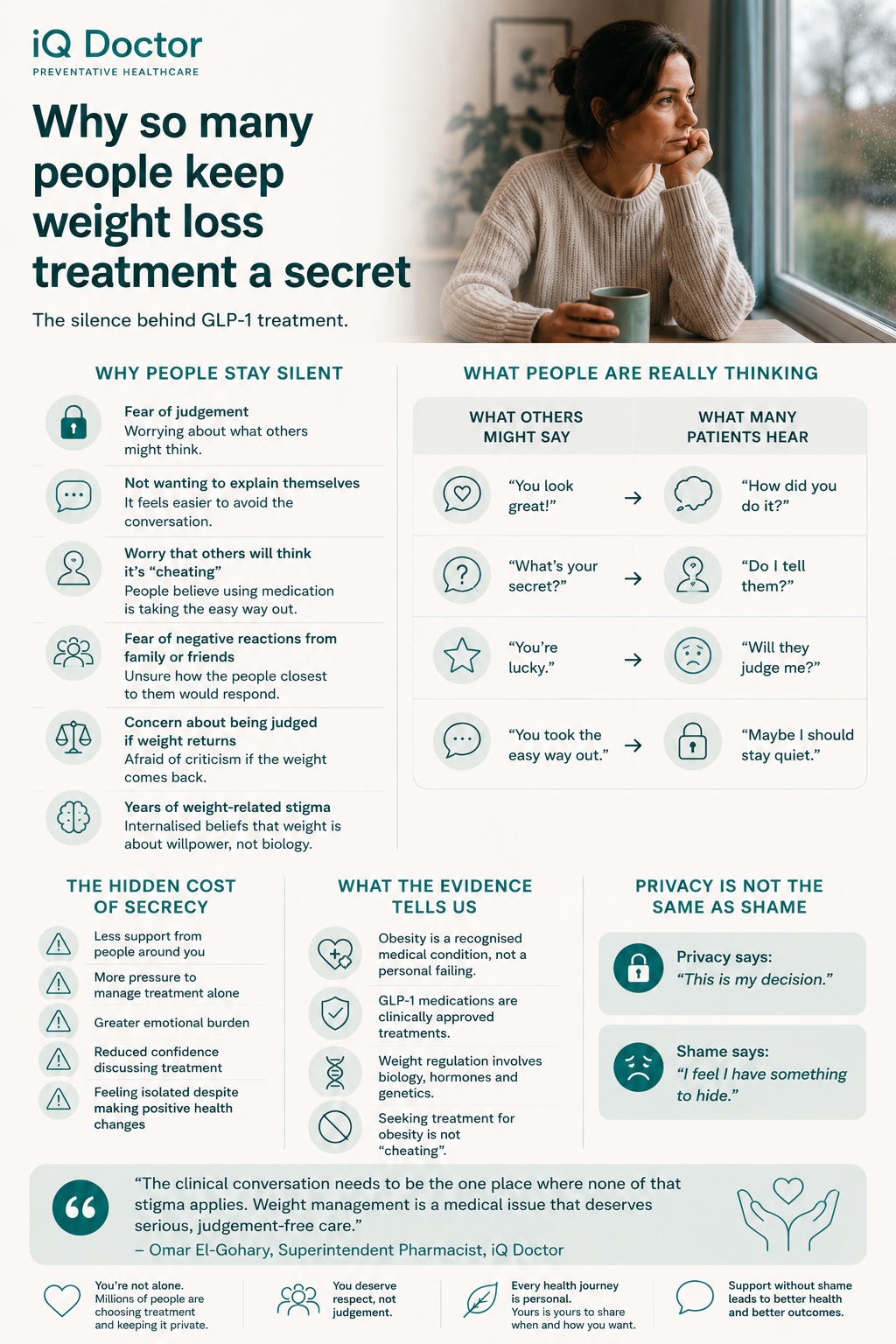
Why so many people keep weight loss treatment a secret
They’ve been using it for three months. Their clothes fit differently. Their energy is better. The constant background noise of food they’d lived with for years has, for the first time, gone quiet.
And they haven’t told a single person.
Not their partner, not their best friend, not the colleague who’s noticed they look different and keeps asking what they’re doing. A conversation has been carefully deflected, redirected, or simply avoided so many times it has become second nature.
This is not unusual. Across the UK and globally, as GLP-1 medications like semaglutide and tirzepatide become increasingly prescribed for obesity treatment, a striking and medically significant pattern has emerged: a large proportion of people using these treatments are keeping it a secret. In some surveys, the majority.
There are reasons for this, and they are understandable. But there is also a cost to individuals, to clinical relationships, and to the broader conversation about what obesity actually is, and what its treatment should look like.
In this article, I want to explore why the secrecy exists, what drives it, and why I think opening up the conversation, however gradually and on your own terms, matters.
What this article covers
- Why so many people keep weight loss treatment private
- The stigma behind the silence, and where it comes from
- The health consequences of secrecy in treatment
- What people fear, and whether those fears are warranted
- How the clinical conversation should feel different
- Why treating obesity is not cheating
The scale of the silence
The numbers are striking. A 2023 survey conducted in the United States found that more than half of people using GLP-1 medications for weight management had not disclosed this to people in their personal lives, including in some cases their own family members.(1) UK data shows similar patterns, with many patients describing a conscious decision to keep treatment private, not from their prescriber, but from the people around them.(2)
This is worth sitting with for a moment. We are talking about a generation of people managing a recognised medical condition, using a clinically approved treatment, and feeling that they cannot talk about it.
They are not keeping it secret because the treatment is dangerous or illicit. They are keeping it secret because the social environment around weight, and around the decision to use medication to address it, remains deeply complicated.
When I speak to patients at iQ Doctor, a version of this comes up regularly. Someone will describe weeks or months of treatment, meaningful changes in their health and how they feel, and then mention almost in passing that nobody in their life knows. The word they most often reach for is ‘ashamed.’ Sometimes ‘embarrassed.’ Often, simply ‘I don’t want to deal with the reaction.’
That last one is important. The secrecy is not always about personal shame. Sometimes it is a calculated decision to protect a treatment that is working from a social environment that might undermine it.
Where the stigma comes from
The stigma around weight loss medication is not a straightforward thing. It comes from multiple directions simultaneously, and they do not always agree with each other.
The first and most pervasive is the cultural belief that weight is primarily a matter of personal responsibility, that being larger is the result of insufficient discipline, and that losing weight through medication is therefore a form of cheating. This belief is so deeply embedded in how many people think about weight that it often operates below the level of conscious reasoning. People who hold it are not necessarily unkind. They have simply absorbed a message that has dominated public and clinical discourse for decades: that you just need to try harder.(3)
The research does not support this framing. Obesity is a complex, multifactorial condition involving genetic predisposition, neurobiological factors, hormonal regulation, socioeconomic circumstances, and environmental influences.(4) The idea that it is simply a failure of character has been comprehensively challenged by the evidence. But evidence and cultural belief do not always move at the same speed.
The second source of stigma, and one that is particularly relevant to GLP-1 medications specifically, is the perception that these drugs are a shortcut used by people who want results without effort. This has been amplified considerably by media coverage that has disproportionately focused on celebrity use, cosmetic outcomes, and the experience of people who are not clinically obese using medication for aesthetic weight loss.(5)
That coverage has created a version of these medications in the public imagination that is quite different from what they are clinically designed to do. For someone using semaglutide or tirzepatide because they have a BMI over 30, because they have type 2 diabetes or cardiovascular risk factors, because every other approach they have tried has failed, the context is completely different. But the social association can follow them regardless.
And then there is the fear of appearing weak, which maps differently onto different people. For many men in particular, seeking any form of health intervention that involves admitting they cannot simply push through a problem carries its own particular weight. Weight loss medication intersects with both the general male reluctance to seek help and the specific cultural shame around weight.
If you’re using or considering weight loss treatment and wondering whether it’s something to be private about, a conversation with a clinician is a good starting point. At iQ Doctor, our UK-based clinical team provides confidential consultations for weight management. We understand the context. There is no judgement here.
Explore weight loss treatment at iQ Doctor
What people fear and whether those fears are warranted
When patients describe why they have kept their treatment private, the reasons tend to cluster into a few recognisable categories.
The most common is the fear of judgement from people they care about. The worry that someone close to them will diminish what they are achieving (‘oh, it’s just the injection doing the work’), or will treat the choice as a moral comment on their previous behaviour (‘you should have done this years ago’). Neither of those responses is helpful, and both are common enough that the fear of encountering them is rational.
The second is the fear of having to justify themselves, of entering conversations they feel unprepared for or conversations that require them to explain the complexity of their relationship with food, their body, and their health in a context where the other person simply does not have the background to receive that well.
The third, which comes up more often than you might expect, is the fear that if treatment stops working or they regain weight, the secrecy becomes harder to maintain and the exposure more complete. There is a kind of pre-emptive self-protection in not telling people, so that if things do not go as hoped, there is no one who knows to be disappointed.
None of these fears are irrational. They reflect real patterns in how weight is discussed socially, and real risk assessments based on previous experience. The problem is that acting on them, while understandable, can have consequences.
The health consequences of keeping treatment secret
Secrecy around medical treatment is not a neutral choice. It has documented effects on health outcomes, and those effects are worth understanding.
The first is adherence. People who keep their treatment private are less likely to have the social support that helps them stay consistent with it. Medication adherence in chronic conditions improves significantly when patients have at least one person in their life who knows about their treatment and engages with it supportively.(6) Keeping a medication regime entirely to yourself, managing it around other people’s presence, navigating meals and social occasions without context this adds a layer of cognitive and emotional load that makes sustained adherence harder.
The second is the clinical relationship. Patients who feel ashamed of their treatment are less likely to be fully transparent with their prescriber. They may underreport side effects they feel embarrassed about. They may not raise questions they have because asking feels like admitting something. They may stop treatment without telling their clinical team, or change their approach without consultation. All of this matters for safety and outcomes.(7)
The third is psychological. Living with a significant secret about your own health, managing other people’s perceptions, deflecting questions, is a chronic low-level stressor. For people managing a condition that already has significant associations with shame and self-worth, adding a layer of concealment tends to compound rather than protect against the psychological burden of treatment.(8)
None of this is a suggestion that people should feel obligated to disclose their treatment to anyone. Confidentiality is a right, not a failing. But there is a meaningful difference between choosing not to disclose and feeling unable to. The first is agency. The second is constraint. And constraint tends to carry costs.
Treating obesity is not cheating
I want to address this directly, because it is at the heart of a lot of the shame I encounter.
GLP-1 receptor agonists do not lose weight for people. What they do is address a specific physiological barrier that many people with obesity experience: the neurological and hormonal drivers of appetite dysregulation that make sustained dietary change extremely difficult to maintain over time.(9) Many people using these medications describe, often for the first time in their adult lives, not thinking about food constantly. Not because they lack discipline, but because a biological signal that was previously running at full volume has, finally, been turned down.
If someone had a condition that affected their ability to regulate blood pressure, and they took medication that helped regulate it, we would not describe that as cheating on healthy living. We would describe it as treatment. The same logic applies here, but the cultural framework around weight has not yet caught up with the clinical one.
The evidence for this is clear and growing. The pathophysiology of obesity involves leptin resistance, ghrelin dysregulation, altered dopamine signalling and genetic factors that interact with environment in ways that make it a chronic, relapsing condition for many people, not a problem of character.(4) Treating it medically is appropriate. It is evidence-based. It is, increasingly, what guidelines recommend.
The shame is not medically justified. But it is socially real. And until the cultural framing catches up with the clinical understanding, people are navigating that gap largely alone.
“The patients I speak to who are keeping their treatment private are often managing something genuinely difficult: a condition that is hard to treat, in a social environment that makes them feel the need to hide the treatment that is actually working. The clinical conversation needs to be the one place where none of that applies. At iQ Doctor, we treat weight management for what it is: a medical issue that deserves serious, stigma-free clinical attention.”
Omar El-Gohary, Superintendent Pharmacist, iQ Doctor
How the clinical conversation should feel different
One of the reasons patients keep treatment private from their prescriber, as well as from people in their personal lives, is that they have had previous clinical experiences in which weight was handled unhelpfully. Being told to eat less and exercise more without any acknowledgement of why that has not worked. Having weight raised in the context of an entirely unrelated appointment. Feeling that a clinician’s response was impatient, dismissive, or that the scale was treated as a moral rather than a clinical instrument.
Those experiences are common, and they create a template for what clinical conversations about weight feel like, one that many people are understandably reluctant to return to.
It does not have to be that way, and it should not be. A proper clinical conversation about weight management acknowledges the complexity of the condition. It does not ask people to justify why previous attempts have not worked. It looks at the full picture: current weight, metabolic health, medical history, previous interventions, and what the individual’s own goals and priorities are. It gives information about what treatment options exist and what the evidence says, without attaching a moral valuation to any of them.
That conversation is available. The clinical tools are considerably more effective than they were even five years ago. The barrier, more often than not, is not access to treatment. It is the expectation, based on previous experience, that the conversation will not be worth having.
I would encourage anyone reading this who has been avoiding that conversation for that reason to try again, in a setting where weight management is taken seriously as a clinical issue. Because the treatment landscape has changed, and because you deserve a clinical relationship where you do not have to carry shame into the room.
What practical steps look like
You do not owe anyone a disclosure
Your medical treatment is your business. You are entitled to privacy about your health in every relationship, including close ones. If you choose not to tell people what you are taking, that is a valid choice, and it does not need to be justified. The goal is not to make everyone around you comfortable with your treatment decisions. The goal is for you to manage your health effectively.
But consider who you trust
There is a meaningful difference between not disclosing widely and having nobody at all who knows. One person who understands what you are doing and why, who can offer practical support and normalise the experience rather than complicate it, tends to make a significant difference to adherence and psychological wellbeing.(6) You do not have to tell everyone. But consider whether there is one person in your life who might be capable of receiving this well.
Be honest with your clinical team
Whatever you decide about disclosure in your personal life, the most important place to be fully transparent is with your prescriber. That means telling them about side effects, including ones that feel embarrassing. Telling them if you have missed doses or changed the way you are taking medication. Raising questions even when asking them feels like admitting something. Your clinical team needs accurate information to support you safely. Their role is clinical, not evaluative.
Notice the difference between privacy and shame
Privacy is a conscious choice about who has access to information about you. Shame is the feeling that what you are doing is wrong. They can look similar from the outside but they have very different effects. If keeping your treatment private feels like a relief, that is privacy. If it feels like a burden you carry every day, that is worth examining, both for its own sake and because it tends to have consequences for how you engage with treatment.
Ready to have the conversation without the judgement?
iQ Doctor offers confidential, clinician-reviewed weight management consultations with UK-registered prescribers. If treatment is clinically appropriate, we will support you safely, thoroughly and without stigma.
Start a consultation at iQ Doctor
Frequently asked questions
The following questions are answered with reference to current clinical understanding. If you have specific concerns about your own health, please speak to a healthcare professional.
Why do so many people keep weight loss medication private?
The secrecy is largely driven by social stigma around both obesity and the use of medication to treat it. Many people fear being judged for ‘taking the easy way out’ or having their achievement diminished. Others are protecting themselves from reactions they have experienced before. Research suggests that more than half of people using GLP-1 medications have not disclosed this to people in their personal lives.(1)
Is it medically necessary to tell people you are using weight loss medication?
No. Your medical treatment is confidential and you are not obligated to disclose it to anyone other than your clinical team. However, having at least one trusted person who knows about your treatment can meaningfully support adherence and psychological wellbeing. The most important disclosure is to your prescriber, who needs accurate information to support you safely.(6)
Is using GLP-1 medication for weight loss ‘cheating’?
No. GLP-1 medications address specific neurobiological and hormonal drivers of appetite dysregulation, which are among the primary physiological mechanisms that make sustained weight loss difficult for people with obesity. Treating a medical condition with medication is clinically appropriate, evidence-based, and increasingly recommended in international guidelines. The idea that it constitutes cheating reflects cultural beliefs about weight that are not supported by the science.(3,4)
How does keeping treatment secret affect health outcomes?
Research indicates that secrecy around medical treatment is associated with lower adherence, reduced transparency with clinical teams, and higher psychological burden. Patients who feel ashamed of their treatment are less likely to report side effects, ask questions, or seek support when they need it, all of which can affect safety and outcomes.(6,7,8)
Why do people feel ashamed of weight loss medication when they wouldn’t feel ashamed of medication for other conditions?
The stigma around weight is unique in its cultural depth and persistence. Weight is widely perceived as a matter of personal choice and discipline in a way that other medical conditions are not, which means that treating it medically is interpreted by some people as an admission of personal failure rather than a clinical decision. This framing is not supported by the evidence on obesity’s aetiology but remains culturally dominant.(3,4)
What if someone close to me is dismissive of my treatment?
That is a genuinely difficult situation, and one that many people using these medications have navigated. You do not have to defend your treatment to anyone. If someone’s response is unhelpful, it is entirely reasonable to redirect the conversation or decline to continue it. Your treatment decision was made with clinical guidance. It does not require social ratification to be valid.
When should I seek clinical support for weight management?
If your weight is affecting your health, your quality of life, or has not responded to lifestyle interventions alone, a clinical consultation is appropriate. Obesity is a recognised medical condition, and its treatment: including pharmacological options where clinically indicated, is a legitimate and well-evidenced pathway. You do not need to have exhausted every possible effort before seeking medical support.
References
- Wharton S, Lau DCW, Vallis M, et al. Obesity in adults: a clinical practice guideline. CMAJ. 2020;192(31):E875–E891. [Survey data on disclosure of GLP-1 use referenced in associated patient behaviour literature; see also Puhl RM, 2020.]
- Puhl RM, Himmelstein MS, Pearl RL. Weight stigma as a psychosocial contributor to obesity. Am Psychol. 2020;75(2):274–289. Available from: https://doi.org/10.1037/amp0000538
- Brownell KD, Kersh R, Ludwig DS, et al. Personal responsibility and obesity: a constructive approach to a controversial issue. Health Aff (Millwood). 2010;29(3):379–387. Available from: https://doi.org/10.1377/hlthaff.2009.0739
- Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev. 2017;18(7):715–723. Available from: https://doi.org/10.1111/obr.12551
- Capehorn MS, Catarig AM, Furberg JK, et al. Efficacy and safety of once-weekly semaglutide 1.0mg vs once-daily liraglutide 1.2mg as add-on to 1–3 oral antidiabetic drugs in subjects with type 2 diabetes. Diabetes Metab. 2020;46(2):101–109.
- DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol. 2004;23(2):207–218. Available from: https://doi.org/10.1037/0278-6133.23.2.207
- Burgess DJ, van Ryn M, Dovidio J, Saha S. Reducing racial bias to reduce health disparities: the role of targets. Am J Public Health. 2007;97(5):799–801.
- Pearl RL, Puhl RM. Weight bias internalization and health: a systematic review. Obes Rev. 2018;19(8):1141–1163. Available from: https://doi.org/10.1111/obr.12701
- Drucker DJ. The biology of incretin hormones. Cell Metab. 2006;3(3):153–165. Available from: https://doi.org/10.1016/j.cmet.2006.01.004
Reviewed By

Omar El-Gohary
CEO & Superintendent Pharmacist, iQ Doctor - Registration Number 2059792.
Omar is passionate about developing healthcare technology to empower our patients.